About 6 months ago, I wrote this article: Post-Corona Trends: Life After COVID-19.
At the time, there wasn’t much data available on Covid-19, but the picture seemed bleak. I accepted this picture at face value – in fact, I was preparing for a pandemic while the media and government were saying not to worry:
Watching the Bill Gates Ted Talk a few years back had sowed the seed in my mind that pandemics are not only perfectly possible but pretty much inevitable. Viruses mutate all the time and, despite being against international law, the potential of biological weapons is so huge that you have to expect nation states are at the very least researching them. It seemed only a matter of time before a disease would emerge that posed an existential threat to the human race.
But, in the weeks that followed my initial post, more data on Covid-19 came in. With hindsight it’s clear that Covid-19 wasn’t as deadly as many feared. In fact, it’s not even in the same ballpark.
What follows below is my updated take on Covid-19. I realise the points here aren’t particularly new, but I wanted to write this update because I don’t want to play any part – however small – in perpetuating hysteria and a ‘new normal’ of disproportionate fear, snitching, and tyranny.
Flattening the curve
Early on in the Covid-19 pandemic the emphasis was on ‘flattening the curve’. Measures to prevent the spread of the virus – social distancing, working from home, avoiding social gatherings, and eventually stay at home orders (lockdowns) – would avoid completely overwhelming the health system.
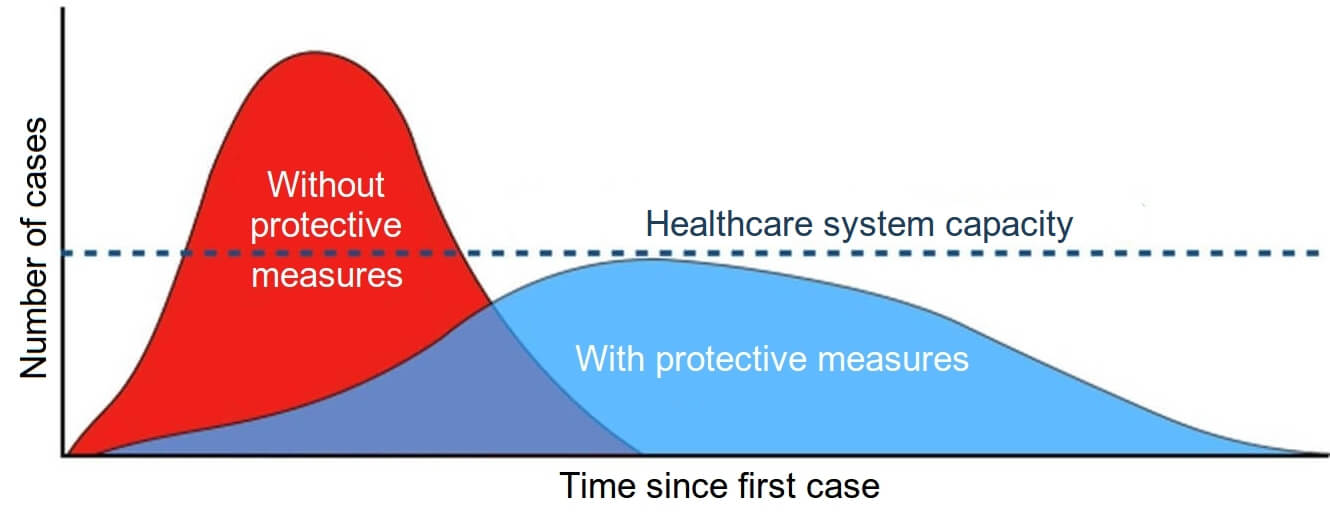
It was argued that without these measures doctors would have to make heart-wrenching triage decisions. Compound growth would lead to a sharp spike in cases and people would very quickly be dying in hospital corridors for lack of resources to treat them all.
“For an uncontrolled epidemic, we predict critical care bed capacity would be exceeded as early as the second week in April, with an eventual peak in ICU or critical care bed demand that is over 30 times greater than the maximum supply in both [the UK and the USA]. The aim of mitigation is to reduce the impact of an epidemic by flattening the curve, reducing peak incidence and overall deaths.”
At the time, it seemed most people were fully behind these measures to flatten the curve. Although unprecedented, policies such as lockdowns would buy the health system precious time and save thousands of lives. It was impressive to see ordinarily bureaucratic organisations spring into action and make use of this time to, for example, construct the NHS Nightingale hospitals in mere days.
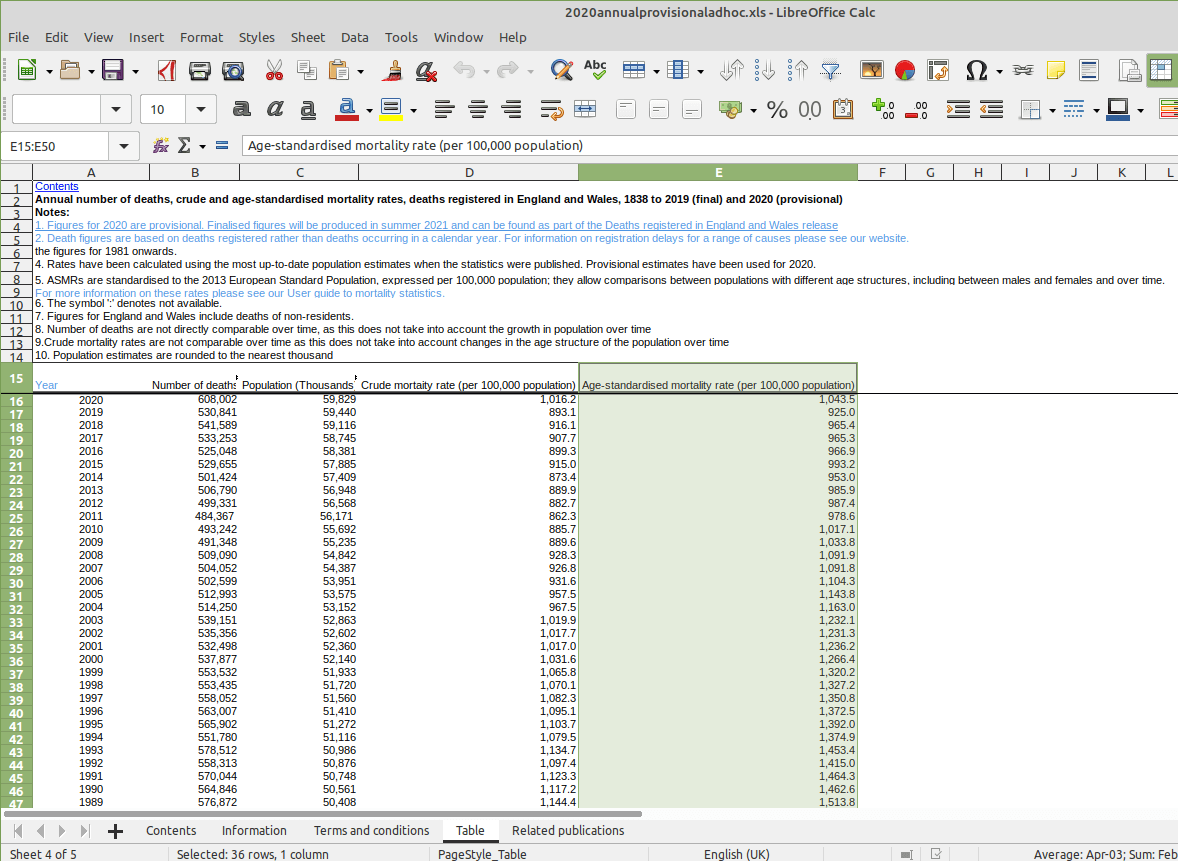
Thankfully, it turned out the curve was nowhere near as steep as the now infamous Imperial College model predicted. Hospital capacity was not exceeded by even 1% – let alone 30x, as the early models predicted – and the Nightingale hospitals were not needed:
“But such high demand for intensive care never materialised. Just 51 patients have been treated at the 4000 bed medical facility situated in the refurbished Excel Centre in London’s Docklands since it opened. Nightingale units in Birmingham and Harrogate have not treated a single patient, while a facility in Manchester has had just a handful of admissions.”
– Covid-19: Nightingale hospitals set to shut down after seeing few patients, BMJ
Even with hindsight, I still think the decision to construct the NHS Nightingale hospitals was justified. You can only act on the knowledge you have at the time, and the information available in late March suggested the excess capacity would be needed. It was one of those situations where it’s better to prepare and not need something than not to prepare and be left wanting.
So, thankfully, we avoided overwhelming the health system – by a considerable margin. And yet despite this, UK authorities are still imposing strict restrictions in October 2020. These strict restrictions were initially framed as temporary measures to ‘flatten the curve’. Now, though, the goalposts have completely moved and the justification for these measures is to prevent the spread of Covid-19 – a justification that can be used indefinitely!
And as more data comes in, this justification looks increasingly weak in proportion to the danger.
Putting the risk in perspective
“A substantial number of people still do not feel sufficiently personally threatened… The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging.”
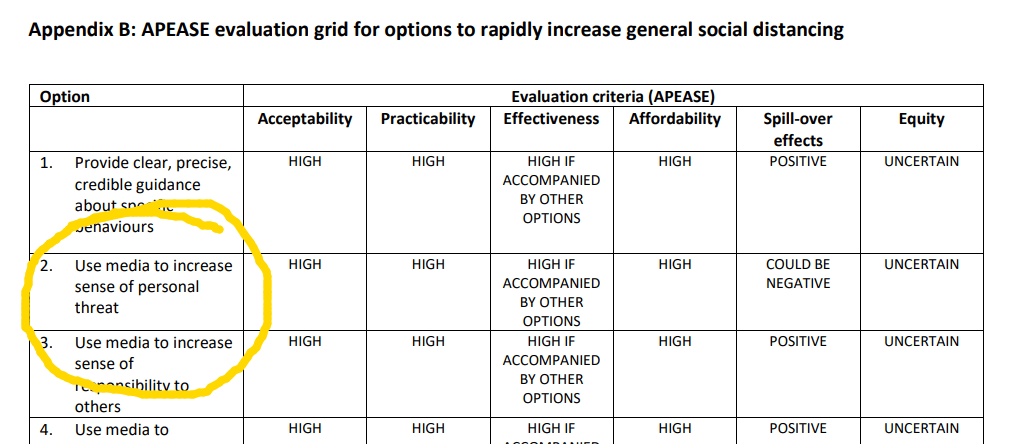
– extracts from a March 2020 paper by the UK Government advisory body SAGE
Given these unprecedented restrictions and the hysteria whipped up by the media and authorities, I strongly suspect most people overestimate how dangerous Covid-19 is – likely by several orders of magnitude.
The table below is from the Centers for Disease Control and Prevention’s (CDC) COVID-19 Pandemic Planning Scenarios:
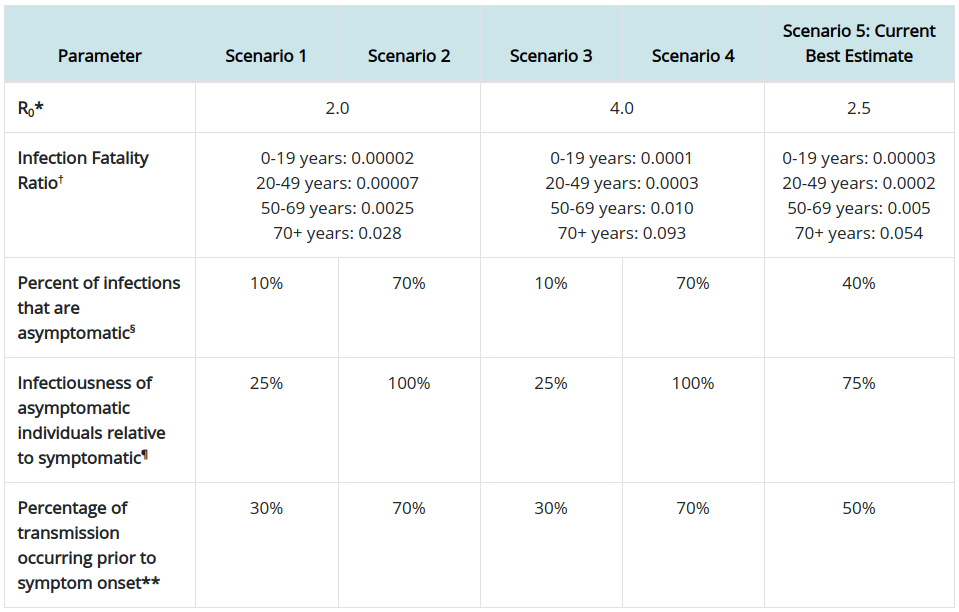
Scenario 5 (the far right column) contains the current best estimates for the infection fatality ratio (IFR) – i.e. if you contract Covid-19, how likely it is that you’ll die. The IFR is presented as a decimal here, and converting it to a survival rate % (i.e. how likely you are to survive if you contract Covid-19) we get the following figures:
| Age | Survival Rate |
| 0-19 | 99.997% |
| 20-49 | 99.98% |
| 50-69 | 99.5% |
| 70+ | 94.6% |
The notion that Covid-19 is only serious for the elderly and those with underlying health conditions turns out to be entirely accurate. Of course, there are anecdotal examples of healthy 20 year olds killed by the virus, but these are rare outliers. I’m sure there are unfortunate people under 40 who’ve died from Alzheimer’s – but this doesn’t mean the average 35 year old should consider themselves at risk.
For comparison, the survival rate of regular flu is roughly 99.9%. This is an average and so, like the table above, you can expect that figure to be higher or lower depending on age (and other risk factors). You can nitpick the exact numbers if you like, but the point is this: The IFR of Covid-19 is in the same ballpark as seasonal flu. It’s not orders of magnitude more deadly like you would expect given policy responses. Covid-19 is certainly not the Black Death – and it’s not even the Spanish Flu.
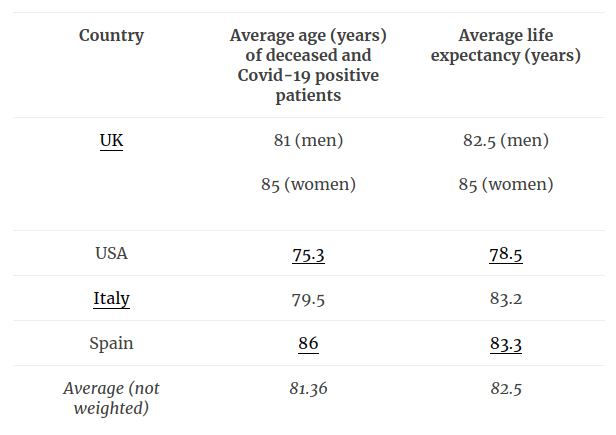
The fact that Covid-19 is pretty much only deadly for the elderly (and those with underlying health conditions) is further illustrated by comparing the average age of people who die of Covid-19 with the average life expectancy:
| Country | Average age (years) of deceased and Covid-19 positive patients | Average life expectancy (years) |
| UK | 81 (men)
85 (women) |
82.5 (men)
85 (women) |
| USA | 75.3 | 78.5 |
| Italy | 79.5 | 83.2 |
| Spain | 86 | 83.3 |
| Average (not weighted) | 81.36 | 82.5 |
I can already hear the objections for pointing this simple fact out: “Oh, so you think we should just let old people die then? That their lives don’t matter?”
Obviously not. I have elderly relatives and would be heartbroken if they died from Covid-19. But I would be heartbroken if they died from anything! And, unfortunately, the older you get, the greater your chance of dying from something gets:
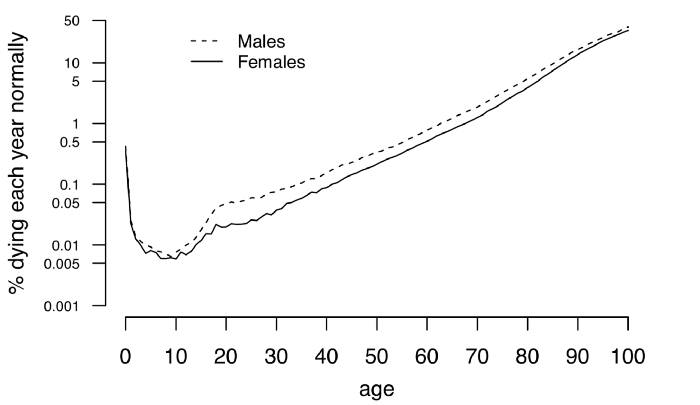
Early on in the pandemic, University of Cambridge statistician Sir David Spiegelhalter wrote a great article comparing the risk of dying from Covid-19 with normal risk in a given year. Sir David describes how your chance of dying from the virus – that’s if you’re unlucky enough to contract it in the first place – is roughly the same as your chance of dying from something in any given year.
“So, roughly speaking, we might say that getting COVID-19 is like packing a year’s worth of risk into a week or two.”
– How much ‘normal’ risk does Covid represent?, Sir David Spiegelhalter
And so, because older people have a higher risk of dying in general, they also have a higher risk of dying from Covid-19.
Obviously you don’t want to increase the risk of you or your loved ones dying unnecessarily. But does this mean we should reduce all speed limits to 5mph so nobody ever dies in traffic accidents? Or ban sugary and fatty foods so nobody dies from heart disease? Of course not!
Good public health policy is in proportion to the risk it prevents and, now that we have more data on Covid-19, it is clear that the extremity of the policies is not in proportion to the severity of Covid-19.
I’d even go further and suggest Sir David’s already reassuring analysis is overstating the risk of dying from Covid-19. In his article, which was written in March 2020, Sir David uses the Imperial College IFR numbers – numbers that are significantly higher than the more recent and more accurate CDC figures posted above. So, rather than packing a year’s worth of risk into a week or two, contracting Covid-19 might be more like packing 6 months worth of risk into a short space of time! Of course it’s possible you might die in the next 6 months, but do you let that paralyse you into staying home forever?
And keep in mind this 6 month’s worth of risk only applies if you actually contract Covid-19 in the first place!
Consequentialist concerns
There’s been some debate (although not in Parliament, where government and ‘opposition’ quibble only over petty details) about whether the draconian policy responses to Covid-19 resulted in a net gain or a net loss for society.
Defenders of lockdowns argue they are necessary to avoid loss of life. However, this argument was far more powerful back in March when it seemed that without ‘flattening the curve’ the health system would be completely overrun, causing otherwise preventable deaths. As mentioned, though, Covid-19 turned out to be far less deadly than initially feared and so it seems highly unlikely we would ever have exceeded health system capacity – especially not to the degree that was initially predicted.
The argument that lockdowns are a net positive becomes weaker still when you consider that lockdowns don’t eliminate the virus but instead only delay its progress. This means that, rather than preventing deaths, lockdowns just postpone many until some point in the near future – and at huge costs to society.
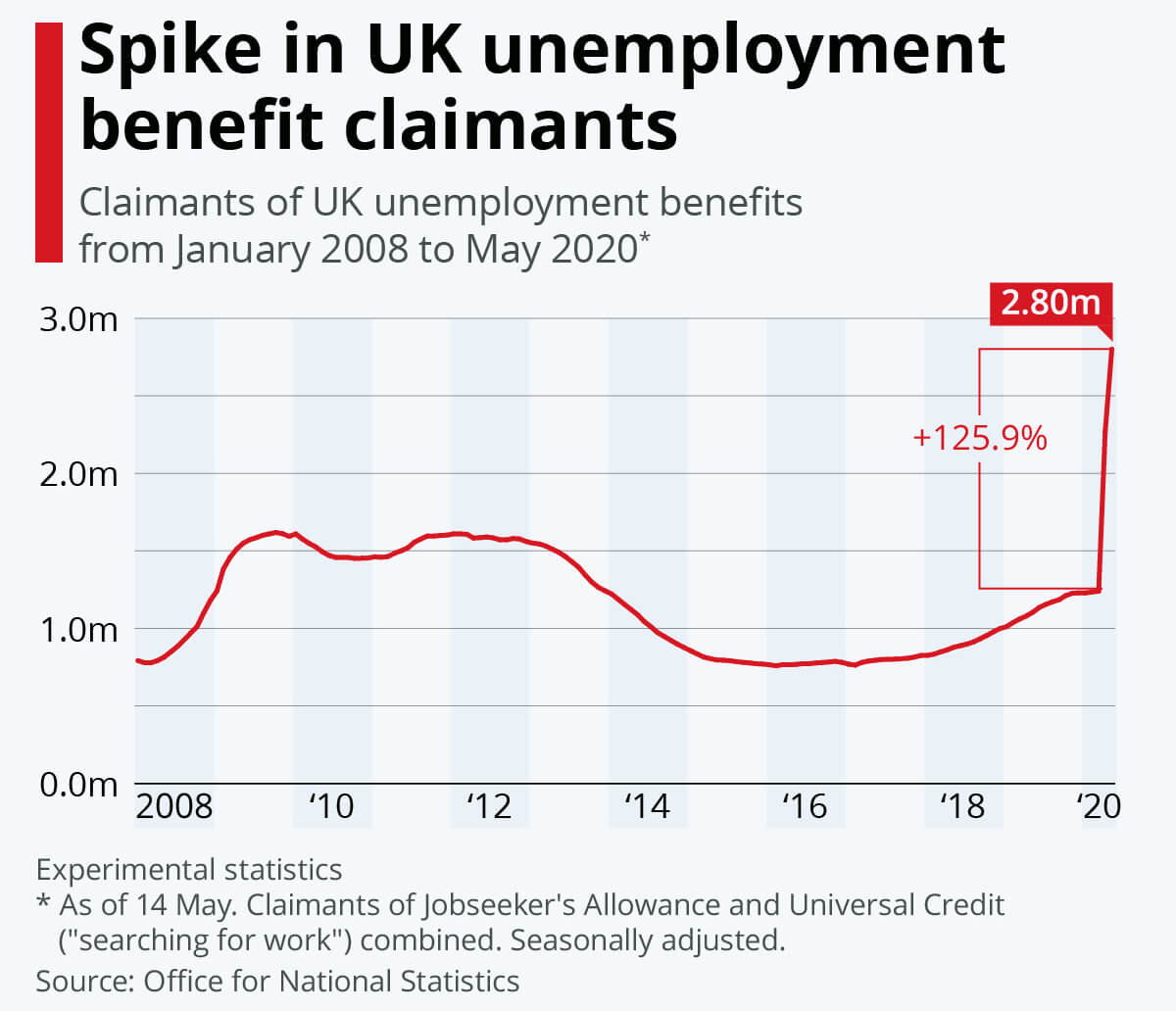 These costs include deaths as a result of these policies, such as those caused by changes to healthcare practices (potentially as many as 185,000). There are, of course, significant economic costs too: Many businesses have gone under, unemployment has skyrocketed, and taxpayers will be paying off debt incurred to fund furlough and other such schemes for decades to come (poverty like this also reduces life expectancy). There’s also less tangible effects such as reduced mental health and the long term impact of taking so many children out of school for so long.
These costs include deaths as a result of these policies, such as those caused by changes to healthcare practices (potentially as many as 185,000). There are, of course, significant economic costs too: Many businesses have gone under, unemployment has skyrocketed, and taxpayers will be paying off debt incurred to fund furlough and other such schemes for decades to come (poverty like this also reduces life expectancy). There’s also less tangible effects such as reduced mental health and the long term impact of taking so many children out of school for so long.
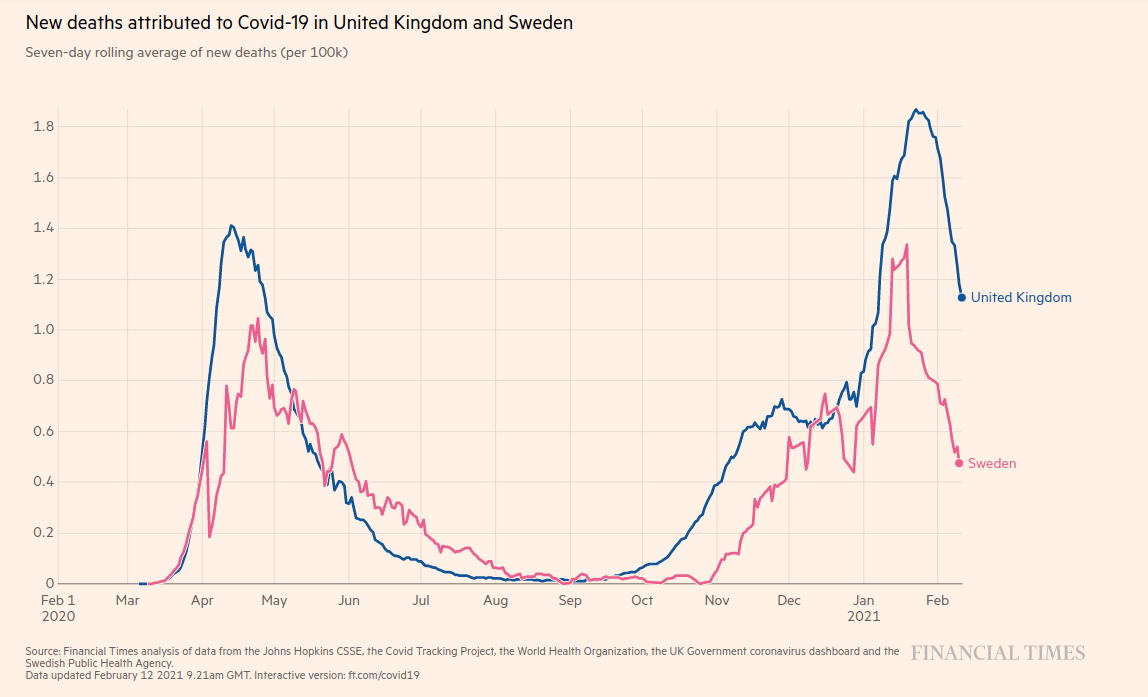
Despite all this, it’s impossible to definitively prove whether lockdowns resulted in a net gain or a net loss for society. Each side in this debate gets to point to an unfalsifiable counterfactual world: Sceptics describe how much better things would be if we didn’t have the lockdown, and advocates describe how much worse it would be if we didn’t. Unlike a lab test, however, we can’t run the experiment twice to compare. At best, we can compare between countries. I might, for example, point to the lower per capita death rate in Sweden (no lockdowns) compared to the UK – but there are so many variables to control for with such comparisons that each side will just end up tweaking these to suit their biases.
My bias is obviously that the extreme response to Covid-19 resulted in a huge net loss for society compared to more moderate measures.
| Cons of lockdown | Pros of lockdown |
|
|
Undermining liberty
But as strong as the consequentialist argument is, the net loss for society is not my main issue with Covid-19 lockdowns. I’m not a utilitarian and I don’t buy into this mentality that everything has to be quantified and justified in economic and consequentialist terms.
The lockdown advocates are both right and wrong in their criticism that “you care more about the economy and money than saving lives!” They’re right that there is more to life than economics and certainly more to life than money. But there’s also more to life than simply being alive like some sort of battery chicken. We should act to preserve life, of course, but not at any price.
And, for me, the loss of freedom is a price not worth paying in this case. Not even nearly.
The British public stood by – and in many cases actively cheered on – as government completely trampled on their rights. In exchange for the false promise of ‘safety’ (from a disease with a >99% survival rate), people simply accepted that authorities could now prevent them from seeing their loved ones, from partaking in activities they enjoy, or from running their ‘non-essential’ businesses.
Look around you: We’ve completely overhauled our way of life. Even now, you can’t meet more than 5 friends. Sports and social events are banned. You can’t go for a drink in the pub after 10pm. And authorities are bringing in ‘Covid Marshalls’ to ensure compliance.
And for what? A bad flu.
Until Covid-19, it was common sense that people should be free to decide their own risks. We don’t ban sugary foods, say, despite the fact that they cause heart disease when consumed in excess. We don’t ban alcohol even though it causes liver damage.
We do, for example, ban heroin – because it’s just that addictive and harmful. Even hardcore libertarians can at least appreciate the rationale: Banning heroin is proportionate to the damage it causes.
 But unlike banning heroin, forcing everyone to stay at home because they might catch a virus with a >99% survival rate (>99.9% in the under 50s) is not proportionate to the risk. Again, the two things aren’t even in the same ballpark.
But unlike banning heroin, forcing everyone to stay at home because they might catch a virus with a >99% survival rate (>99.9% in the under 50s) is not proportionate to the risk. Again, the two things aren’t even in the same ballpark.
The extent to which government has undermined our freedom is completely unprecedented, but the level of danger presented by Covid-19 is not.
Let’s say you’re five times as likely to die from Covid-19 than seasonal flu (you’re not) and twice as likely to contract it. Were you anything like 10% as concerned as you are now compared to 2019? Nevermind the ‘rule of six’, how would you have reacted to a rule of sixty last flu season? Such ideas would have been laughable because they are disproportionate to the risk.
For most people, flu was so far down the list of concerns prior to Covid-19 that it didn’t even register as one. And if you scale that concern up 10x (which is very generous, given the data above) it still doesn’t scratch the surface – much less justify these extreme policies.
Seasonal flu has always been a risk for the elderly and vulnerable and so, yes, we should take extra care to shield them from Covid-19. But even so, government does not have grounds to compel such actions.
Even someone at very high risk – an 85 year old Grandfather with asthma, say – should be allowed to see friends and family if he wishes. It’s his choice. He might prefer to accept the risk and enjoy what time he does have rather than possibly extending that time slightly only to live alone and in fear. What right does anyone have to make that choice for him?
It’s all so inhumane.
Finally, I’m sure there are people who got bent out of shape by my comparisons of Covid-19 to drinking alcohol or driving a car: “But those things aren’t contagious!”
This is basically the objection that freedom to choose doesn’t mean freedom to harm others. However, giving people the freedom to decide risk for themselves – like adults – negates this objection anyway.
 People who are so scared about getting Covid-19 are also free to choose: To stay safely locked up and socially distanced at home. Public policy could – and indeed does – make provision for such people to avoid social contact (especially the vulnerable, which I wholeheartedly support). But beyond this, why should a paranoid few expect everyone else to accommodate their fear of possibly catching a virus with a >99% survival rate?
People who are so scared about getting Covid-19 are also free to choose: To stay safely locked up and socially distanced at home. Public policy could – and indeed does – make provision for such people to avoid social contact (especially the vulnerable, which I wholeheartedly support). But beyond this, why should a paranoid few expect everyone else to accommodate their fear of possibly catching a virus with a >99% survival rate?
Why should you have to stay home because they are scared of getting infected by you? Wouldn’t it make more sense for them to just stay home instead?
This ‘new normal’ meme needs to die. If you agree, please consider signing the Great Barrington Declaration below.
Another Update (24/10/2020)
I really tried to steelman the opposing view while writing this. A few days after posting this, the John Snow memo emerged, which is a sort of anti-Great Barrington Declaration.
The John Snow memo claims “The infection fatality rate of COVID-19 is several-fold higher than that of seasonal influenza” and cites Estimates of the severity of coronavirus disease 2019: a model-based analysis as a source for this. But this paper, like the original Imperial College model, was published in March when there was hardly any data available and uses a tiny sample size. This citation is now totally at odds with the more recent and more accurate IFR numbers from the CDC posted above, which are further supported by a meta-analysis recently posted to the WHO:
“In people < 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%.”
– Infection fatality rate of COVID-19 inferred from seroprevalence data. Article ID: BLT.20.265892
Elsewhere, SAGE has published a supposed rebuttal of the sort of targeted shielding strategy advocated by the Great Barrington Declaration. Below are the key points of the SAGE memo and my replies:
- “It would not be possible to prevent the virus spreading from younger people to older people.”
True. But it “would not be possible to prevent the virus spreading” with lockdowns or draconian policies either. At best, draconian interventions slow the spread, but they also have enormous negative consequences (including loss of life) of the kind mentioned above. Current policies are just delaying the inevitable – and at a massive cost for society.
- “A very large proportion of the population would need to withdraw from daily life for many months, which would have profound negative effect [sic] on them.”
Current policies already have a “profound negative effect” on the entire population that will be felt for years to come. Further, many vulnerable people are “withdraw[ing] from daily life for many months” under the current strategies anyway. What’s even worse is that, despite this, cases are rising anyway! This just underscores my point above that draconian interventions are only delaying the inevitable, and at huge cost to the entire society.
- “An uncontrolled epidemic in younger age groups would have dire consequences for the NHS as well as having unknown long term effects in those infected.”
We were already warned of “dire consequences for the NHS” back in March that never even nearly materialised, as evidenced by the vacant Nightingale Hospitals. This is cause for scepticism, as is the >99.9% survival rate in the under 50s, the low number of deaths relative to cases, and current ICU bed occupancy.
As for “unknown long term health effects”, this is really clutching at straws. You could just as easily argue that a hastily engineered and largely untested vaccine for Covid-19 has “unknown long term health effects”. However, I seriously doubt SAGE will make that same point when a vaccine is available. I’m not saying this because I’m an anti-vaxer, by the way, I’m just pointing out that appeal to “unknown” consequences is a very weak argument.
- “We do not know if long term immunity results from infection with SARS-nCOV-2”
Again, a gap in knowledge (“we do not know”) is used as justification for extreme policies. But there is already good evidence of long term immunity to Covid-19. This paper, published in Cell in August, reports: “Our collective dataset shows that SARS-CoV-2 elicits broadly directed and functionally replete memory T cell responses, suggesting that natural exposure or infection may prevent recurrent episodes of severe COVID-19.” Further, hundreds of millions of people have been infected with Covid-19 already and reports of reinfection are very rare.
But even if there is no long term immunity, so what? We would just have to learn to live with Covid-19 as we’ve always done with so many other cold and flu viruses – again, they’re in the same ball park. More importantly, though, I would refer to my point above about freedom for individuals to decide their own risk of catching a disease with a >99% survival rate.
Third Update (06/11/2020)
On the 1st of November, the Prime Minister announced a month long second lockdown from 5th November.
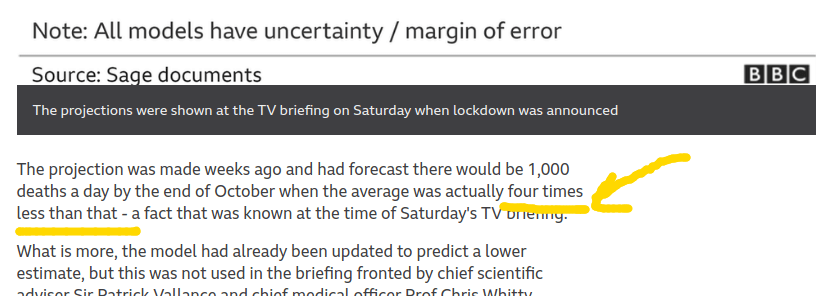
Almost immediately after, the UK Statistics Authority criticised the projections used to justify the lockdowns for using out of date information and significantly overestimating Covid-19 deaths – by 300%!
What’s more, the government didn’t even do an assessment of the costs vs. the benefits for the first lockdown or this most recent one.
The links above are all BBC news and I sense the mainstream is slowly beginning to critically examine the data and policies surrounding Covid-19. But what’s so annoying is how many voices outside the mainstream were doing this months ago. I’m not talking about wild conspiracy theorists or people calling the whole thing a hoax, either – I’m talking about sensible people critically examining the data and drawing different conclusions. However, the discussion in the mainstream – in parliament, in mainstream media, and even social media – has been incredibly one-sided up until this point.
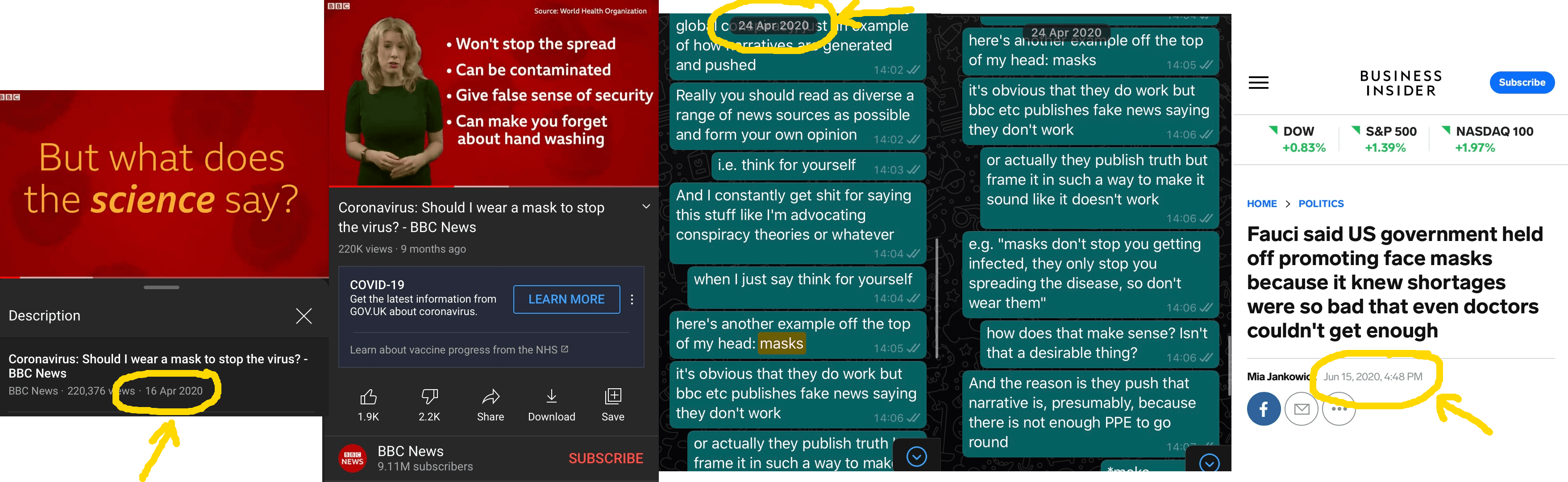
I mentioned above that government and ‘opposition’ quibble over petty details. The two sides have squabbled over to what extent lockdowns are needed and when, but neither side actually questioned whether lockdowns are justified (with a few notable exceptions1,2). Further, the BBC and other legacy media organisations amplified this apparent consensus and rationalised the ‘new normal’ almost without exception. Perhaps most worryingly, social media censored discussion of Covid-19 that questioned the narrative or drew alternative conclusions – however strong the evidence. True opposition and even honest scepticism was stifled and anyone who opposed the Covid-19 dogma was attacked (or silenced) for ‘not following the science’.
 It’s a topic for another day, but this idea of ‘following the science’ is so poisonous. The people who use ‘the science’ in this way are dogmatic – and dogmatism is completely antithetical to what science actually is. Science is not a list of facts to be memorised. Instead, science is a process of sceptically interrogating empirical data to arrive at the truth. Science is also agnostic with regards to values, ethics, and political policy.
It’s a topic for another day, but this idea of ‘following the science’ is so poisonous. The people who use ‘the science’ in this way are dogmatic – and dogmatism is completely antithetical to what science actually is. Science is not a list of facts to be memorised. Instead, science is a process of sceptically interrogating empirical data to arrive at the truth. Science is also agnostic with regards to values, ethics, and political policy.
Even if their conclusions turn out to be wrong, the dissenting voices who scrutinised primary data sources have a far greater right to call themselves ‘scientists’ than the sheep who blindly parrot whatever authority tells them ‘the science’ is.
Fourth Update (01/12/2020)
Probably the most common objection to what I’ve written here is that “without lockdowns the NHS will collapse”. This response fails on multiple levels.
Firstly, it’s now clear that the NHS would not have ‘collapsed’ in any sense of the word. The dramatic word ‘collapse’ would perhaps be applicable in the original scenario predicted by Imperial College where demand for critical care beds exceeded capacity by 30x. But that projection turned out to be inaccurate by several orders of magnitude and now even the most alarmist models – such as those used by the government to justify the second lockdown – don’t predict anything close to this level of demand.
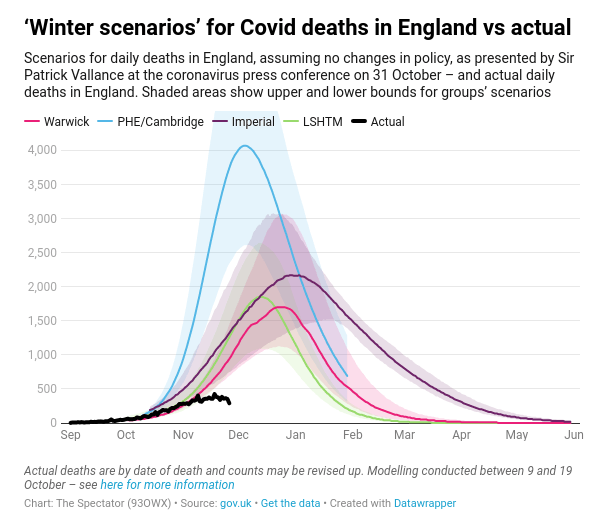
And even then, these newer models still completely overestimate the risk! The graph below shows the actual Covid-19 death rate vs. recent predictions from Warwick, PHE/Cambridge, Imperial, and LSHTM. As you can see, all these models have turned out to be completely wrong:
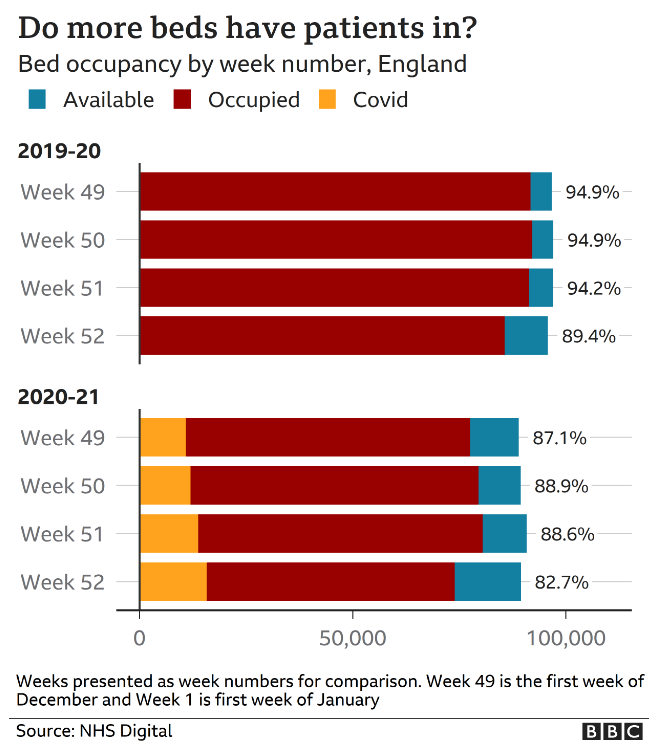
The lack of strain on the NHS is further supported by data on hospital bed occupancy, which is on average lower than the same time last year.
The predictable response at this point is to say that demand for healthcare is low because of lockdowns and other draconian restrictions on freedom. Again, this puts us in the territory of unfalsifiable counterfactual worlds and so I have to argue against a hypothetical armageddon scenario where we didn’t have lockdowns.
As I mentioned above, it’s somewhat pointless arguing against these counterfactual worlds because they’re impossible to prove either way – we can’t run the same experiment twice. UK authorities decided to go with the lockdown option and now we’ll never know for certain what the possible world without lockdown looks like. However, the data that is available does seriously strain the credibility of mathematical models of catastrophe in a no-lockdown scenario. Sweden had no lockdowns or coercive measures – they didn’t even legally mandate asks – and their per capita death rate from Covid-19 is lower than the UK’s. This is despite several models1,2 (using a similar methodology to the UK ones above) that projected demand for ICU beds would exceed capacity by as much as 40x with such an approach. Just like in the UK, though, Swedish ICU capacity was never once exceeded. In other words, when these models have actually been put to the test, they’ve turned out to be totally inaccurate (by several orders of magnitude).
Yes, there are many variables that complicate a direct comparison between Sweden and the UK – population density, average age, average level of fitness, and so on – but such variables have to do a lot of work to explain why the UK would exceed healthcare capacity without lockdowns but Sweden wouldn’t. Instead, the simplest explanation is that the UK projections were just wrong.
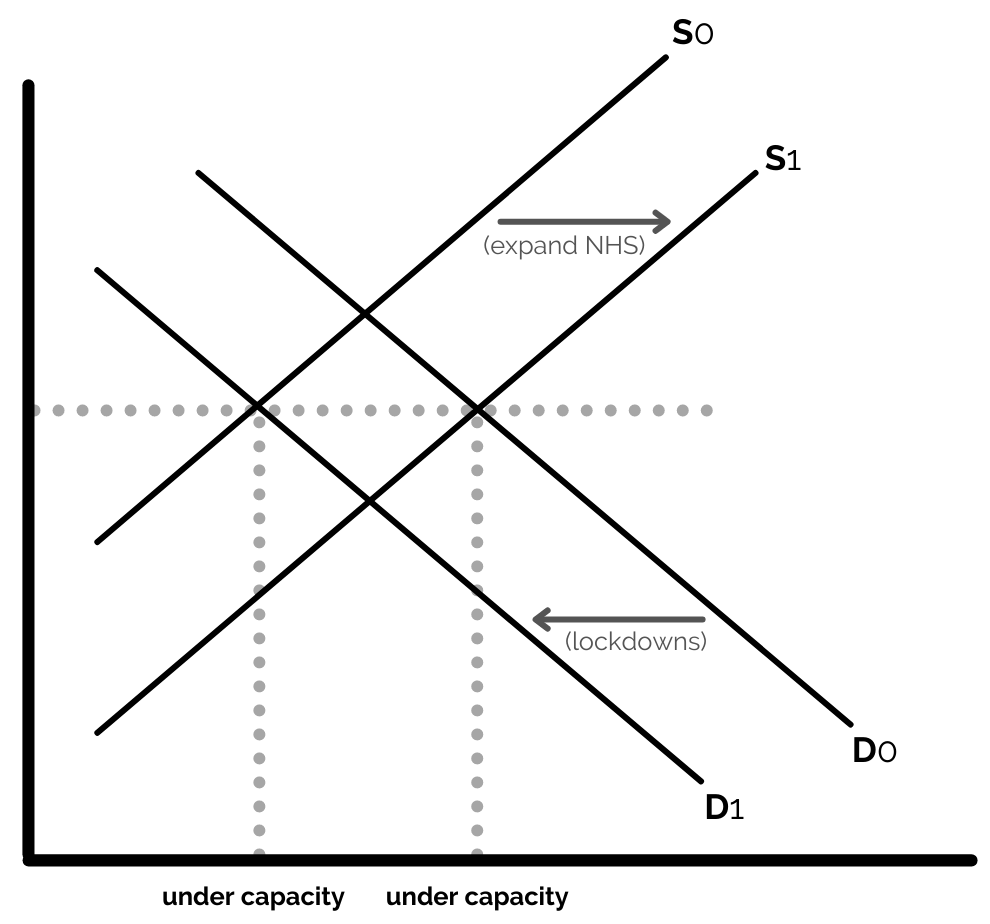
But let’s say we accept that inaction does risk overwhelming the health system – does this justify lockdowns specifically? Well, if our goal is to keep the health system under capacity, there are two ways to do this: Reduce demand or increase supply. Lockdowns seek to avoid overwhelming the system by reducing demand for healthcare services – but at huge cost to society. Wouldn’t it make more sense to respond by increasing supply of healthcare services instead? They’ve already built the Nightingale Hospitals – why not just hire more doctors and nurses to staff them? There’s been more than enough time since March to do so!
This is a situation where the costs vs. benefits of the two strategies are not even close. Whatever the cost of increasing NHS capacity to accommodate Covid-19, it would surely be orders of magnitude less than the cost of lockdowns. The government’s test and trace system alone cost £22 billion, which would be enough to pay £30,000 salaries to more than 350,000 nurses for two whole years. All in, government will borrow almost £400 billion in 2020 to manage Covid-19. Surely that’s many multiples more than would be needed to expand NHS capacity to accommodate a slight increase in demand from Covid-19?!
Whichever way you look at it, lockdowns are not the only way to avoid overwhelming the NHS. But even if they were, it still doesn’t justify them. I don’t buy into this mindset that we must ‘protect’ the NHS at any cost. As people are now daring to point out, the government’s messaging is backwards: The NHS is there to protect the people – not the other way round. Destroying the economy, causing more deaths down the line, and – most importantly – undermining personal liberty is too high a price to pay.
I understand that the NHS is sacred to some people – just like freedom is sacred to me – but it cannot be an absolute value. For some, exceeding NHS capacity by even 1% is unthinkable (even though this already happened as recently as 2018). These people will happily let government impoverish them and take their liberty if they’re told it’s to protect the health service. It’s as though the mere mention of ‘NHS’ casts a spell over these people’s minds such that they will accept any policy – regardless of the evidence.
 But we’re setting a dangerous precedent with these restrictions that fundamentally inverts our conception of government. Instead of the people giving government certain rights, we are normalising and reinforcing the mentality that government is sovereign and that all rights come from government. People talk of government ‘allowing’ us certain freedoms – as though those freedoms are government’s to give. It’s default authoritarianism.
But we’re setting a dangerous precedent with these restrictions that fundamentally inverts our conception of government. Instead of the people giving government certain rights, we are normalising and reinforcing the mentality that government is sovereign and that all rights come from government. People talk of government ‘allowing’ us certain freedoms – as though those freedoms are government’s to give. It’s default authoritarianism.
But liberty should be the default, not authoritarianism. Any restrictions of freedom – particularly as extreme as those we’re seeing – should be challenged and then implemented only when it is beyond any reasonable doubt that such restrictions are absolutely necessary. Instead, there is no impact assessment of these policies and no opposition in Parliament to them.
And yet, many people seem to accept increasingly arbitrary restrictions with an unquestioning and almost gleeful conformity. There are huge swathes of the population who seem desperate for government to control every single aspect of their lives – right down to details as sacred as when and where they can see their family and friends. If someone asks honest questions or expresses concerns about these policies, these same people dismiss them as a ‘Covid denier’ or a ‘conspiracy theorist’ who isn’t following ‘the science’ and wants to kill grandma. It’s bizarre.
I accept that it’s justifiable to restrict liberty in some extreme cases, but Covid-19 is not one of them. Not even nearly. Again, all the most recent data suggests the lethality of Covid-19 is in roughly the same ballpark as flu. It worries me how people are cheering on these unprecedented authoritarian measures – measures enforced by increasingly violent police, by the way – for such a minor threat.
One such basic freedom is the right to protest and the video above shows how the police respond to those who dare to exercise such freedom. This response is particularly concerning in light of today’s vote in the House of Commons, where MPs voted to continue a policy of harsh restrictions unopposed by the ‘opposition’ party, who abstained from voting. So, in other words, you can’t protest against these measures and you can’t even vote against them.
Anyway, in summary, the reasons the “lockdowns are necessary to avoid overwhelming the NHS” argument doesn’t work are:
- Demand for NHS services would likely not exceed capacity without lockdowns (projections used to justify this claim have consistently been wrong)
- But even if Covid-19 meant demand for NHS services would exceed supply, the default response should not be to reduce demand for healthcare via lockdowns. Instead, the more sensible and much less expensive (financially, ethically, and probably in terms of lives lost too) response would be to increase healthcare supply (i.e. build more hospitals and employ more nurses)
- Regardless, exceeding NHS capacity is not some absolute line in the sand that gives government carte blanche to impose whatever restrictions it wants!
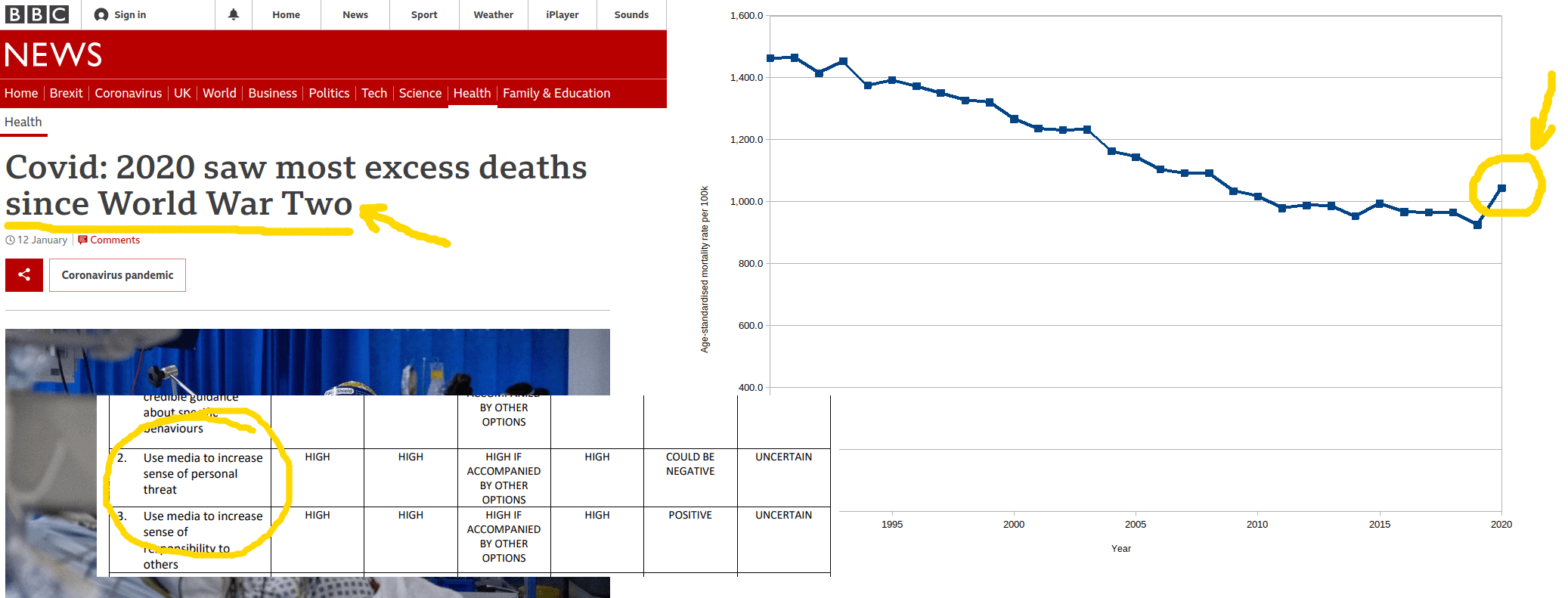
Fifth Update (12/01/2021)
I could use this latest update to once again emphasise how wildly disproportionate this latest round of tyrannical restrictions is, but I’m just repeating myself. At this point, all the facts and figures in the world – the fact that the average age of Covid-19 deaths is basically the same as the average life expectancy, the fact that fewer than 400 healthy people under 60 have died from Covid-19, the >99.9% survival rate in the under 50s – won’t convince some people that the utter destruction of trying (and failing) to prevent these deaths isn’t worth it.
 Facts and figures only go so far. Human beings are not perfectly rational. Emotions and other non-cognitive factors shape our views just as the cognitive factors do – perhaps more so. We are persuaded by narratives, anecdotes, and psychological biases.
Facts and figures only go so far. Human beings are not perfectly rational. Emotions and other non-cognitive factors shape our views just as the cognitive factors do – perhaps more so. We are persuaded by narratives, anecdotes, and psychological biases.
A few years ago, for example, I did a solo skydive. I remember being told the odds of my parachute failing were something like 1 in 700. You have a reserve parachute, though, so the odds of both failing is something like 1 in 490,000. But when the plane hatch opened and I stared out at the green fields thousands of feet below me, the fact that I had a 99.9998% chance of surviving was irrelevant. It was the most fear I’ve ever felt in my life – the reality of the risk didn’t register.
In my original posts, I shared extracts from SAGE report suggesting government use the media to increase fear. This tactic seems to have successfully distorted people’s perception of risk just as fear did when I went skydiving. Further, I’d say these emotional biases are compounded by our biases towards authority (e.g. ‘following the science’) and conformity (e.g. social pressure to wear masks and social shaming of those who don’t follow the rules).
I talked about these biases towards authority and conformity in my post on contrarian investing, and the Covid-19 hysteria definitely shares many similarities with a market bubble. There is a clear parallel between looking at the price of a company as a guide to its value and looking at the Covid-19 policies as a guide to the severity of the disease. It’s natural to think “well, they wouldn’t be doing this if it wasn’t necessary” – but actually look at the data for yourself! Strip out the bias and there’s no way you can make the case for lockdowns from first principles.
Nevertheless, mainstream media outlets support lockdowns pretty much without exception. They constantly emphasise the number of cases – but rarely do you hear about the number of deaths and the prior health status of those who’ve died. You never get any actual analysis that puts these numbers in the context of normal death rates or other flu epidemics1,2. Instead, the media continues to push the narrative that the risk from Covid-19 is totally unprecedented and orders of magnitude worse than any prior epidemic. They also push the narrative that the NHS is on the brink of collapse, despite it being false (or, at the very least, up for debate – especially with regards to appropriate policy responses).
{kind=link}
The latest data from the NHS shows there are many free hospital beds – more so than the same time last year, in fact, despite lower total supply this year. And this is before taking into account the additional capacity afforded by the Nightingale Hospitals – which are on ‘standby’, just in case.
Unfortunately, the NHS is on the brink of ‘collapse’ every year. But nobody called for the total destruction of civil liberties (or anything even resembling these policies) all those other times.



During the past year or so the Covid-19 saga has been going on, I’ve tried looking at this from every angle. I’ve sifted through countless scientific papers, examined multiple datasets, and paid close attention to the news (which is often contradicted by the data). I understand that Covid-19 is worse than regular flu – in particular, more infectious – and that there is some excess mortality (compared to the previous 10 years, say, but not the previous 20, so it depends how you present the data). I’m even willing to accept there could be a risk of overwhelming the NHS, despite figures to the contrary.
But no matter how charitable I am with my interpretation of the data, I cannot find a way to justify this reaction – in particular, legally mandated and enforced lockdowns. MPs seemingly can’t justify them, either: The legislation for all three lockdowns, including this most recent one, states: “No impact assessment has been prepared for these Regulations”.
No matter how I look at this, I can’t conclude anything other than that the response to Covid-19 has been massively disproportionate – a clear overreaction. This was obvious pretty early on (around April, say) and subsequent data has only confirmed this. Lockdown policies are so thoroughly destructive – such an egregious affront to liberty – and yield such little rewards. Yet they were implemented with such little scrutiny.
Not only that, there were so many better alternatives: The focused protection strategy advocated by the Great Barrington Declaration, for example, or using the funds spent counteracting the destructive effects of lockdowns (~£400bn) to increase healthcare supply instead. Even just ‘letting the virus rip’ would have been preferable.
I simply don’t understand what I’m missing here. Either I’m going crazy or the government and the media have got this whole thing totally wrong. At the very least, I would like to hear my views represented, debated, and – if possible – rebutted. But instead:
- My views are not represented in parliament
- My views are not represented in the media
- My views are censored on social media
- And if I try to protest my views, I get arrested by the police
In fact, you don’t have to leave your house – or even break these petty and intrusive rules – to get arrested:
“Protecting public health”.@PoliceScotland stormed into a family home yesterday – on suspicion they had guests around… In fact their seriously ill daughter had just been discharged from hospital.
This is disgraceful. Serious questions must be answered – now. @NicolaSturgeon pic.twitter.com/kNLJhqpynS
— Big Brother Watch (@BigBrotherWatch) January 7, 2021
What else am I supposed to make of all this?
If you’ve ever wondered how you’d have responded living under some oppressive regime, now you know.
Final Update (Summary)
If I could summarise everything above in a single point, it would be this: The reaction to Covid-19 has been (and continues to be) totally disproportionate to the risk.
This is a combination of two claims:
- Covid-19 is not as bad as people generally think
- The reaction to Covid-19 is far more damaging and far less effective than people generally think
At times, I’ve found myself slipping into exaggerations of the two claims above: That Covid-19 is no worse than regular flu, and that lockdowns don’t work at all. But I don’t believe either of these things.
Covid-19 is worse than regular flu – but not that much worse. It’s in the same ball park.
The key facts to support this statement are:
- The survival rate of Covid-19 is far higher than 99% in those aged under 70
- The average age of people who’ve died from (with?) Covid-19 is roughly the same as the average life expectancy
- Fewer than 400 healthy people under 60 died from Covid-19 last year
- Annual excess deaths have been higher many times over the past few decades
- Hospital bed demand never once exceeded supply in 2020
- The threat of Covid-19 has been deliberately hyped by government via the media to create fear
{kind=link}
{kind=link}
I then weigh the risk described above with the costs of these policies, which include:
- Deaths caused by these policies (whether from postponing treatment of other health issues, from reduced physical health caused by keeping people locked up at home, or from reduced mental health from the inhumanity of these restrictions)
- Huge increases in unemployment
- Huge increases in debt
- Huge increases in wealth inequality
- Huge increases in poverty
- Millions of hours of lost education for children
- Violation of liberty and normalisation of authoritarianism
{kind=link}
{kind=link}
To me it’s obvious these costs are not at all commensurate with the risk described previously.
The burden of proof is on those supporting these policies to prove (to a high degree of certainty, really) that they are both effective and proportionate. However, such conclusive evidence is seriously lacking – and there is plenty of evidence to the contrary. At best, the evidence paints an ambiguous picture. And, in the absence of conclusive evidence one way or the other, the default assumption should be freedom. It should take far more than a few academic models (models that have consistently been inaccurate, by the way) to overrule this assumption and pass laws that, for example, criminalise healthy innocent people for seeing their friends and family.
I’ve already emphasised above the high value we should assign to individuals’ freedom to decide their own risk so I won’t stress that point any further here. But the penultimate point – education – is another one I’m particularly upset about. Just like it blows my mind how people can give up so much freedom in exchange for a tiny bit more safety, it blows my mind how people can so readily deprive children of a proper education and normal social interaction with their friends – and for such little reward. ‘The science’ cannot make qualitative judgements on the value of freedom, or of a child’s education, but policy makers and midwit commentators pretend otherwise. However, even on a purely quantitative approach using one single metric – life-years lost – I really struggle to reconcile the costs with the benefits of these policies. And yet despite all this destruction, Covid-19 is still here anyway!
What makes this injustice even worse is that these costs were all man-made and mostly avoidable. I mentioned above that simply doing nothing would have been preferable – but the range of choices was not that stark. There is a sliding scale of policy responses that ranges from doing nothing at all on one end to going full police state at the other end. As you travel along this scale, it seems that increasingly authoritarian measures yield diminishing returns in terms of preventing Covid-19 infections and deaths1,2,3,4,5,6.
Unfortunately – although this should come as no surprise – a certain amount of death is unavoidable.
Preferable compromises could have been:
- Shielding the elderly and vulnerable (e.g. Great Barrington Declaration)
- Emergency increases in healthcare supply to avoid overwhelming the health service
- Mask mandates (assuming masks are effective)
- The UK Department of Health’s own UK Influenza Pandemic Preparedness Strategy 2011
- Some combination of the above
There are many other issues I would like to have covered in this post, but they’d just make it even longer than it already is. Other issues that have been overlooked (and are never included in the softball questions put to government by ‘journalists’) include:
- The high false positive rate of PCR test
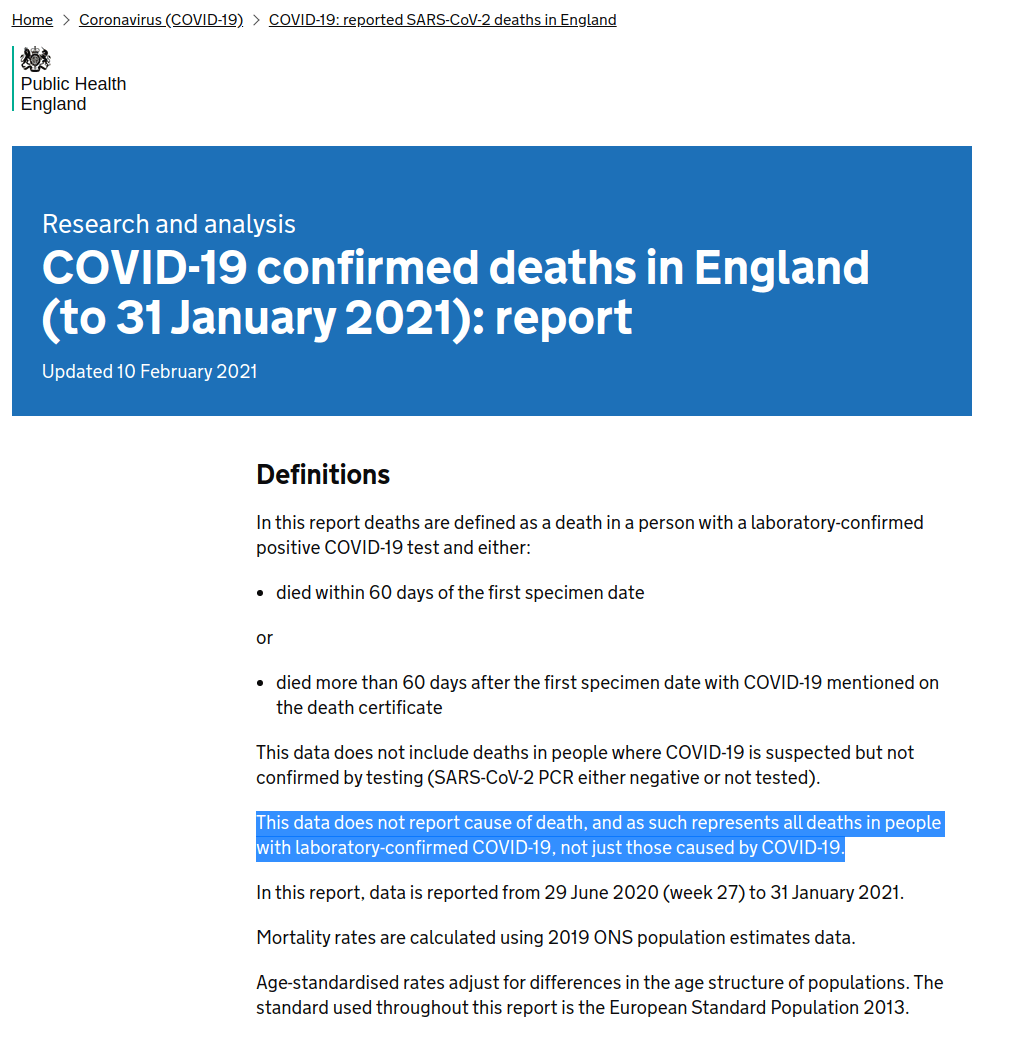
- How Covid-19 deaths are recorded (of vs. with)
- Questions about how much asymptomatic spread there actually is1,2
- The efficacy of drugs hydroxychloroquine and ivermectin in treating Covid-19, and why they seem to have been ignored
{kind=link}
Another topic I avoided in this post is why policy makers got the Covid-19 response so wrong.
I deliberately avoided this topic because such why explanations are always highly speculative and difficult to prove. My main point in this post is simply that policy makers got it wrong. However, some plausible why explanations include:
- Scientific advisers are focused on one single variable – Covid-19 – and do not weigh that against other costs to society
- The public has largely bought in to the Covid-19 narrative and so there are political motivations to be seen as taking tough action against Covid-19 despite it being ineffective/disproportionate to the actual risk
- Incompetence
- Some conspiracy hypothesis (it can’t be ruled out, given the scale of this overreaction compared to how easy it is to draw alternate conclusions from even a cursory examination of data)
- Some combination of the above
Finally, if you think it’s impossible the experts could have got it so wrong and some random person on the internet could have got it right, don’t! Firstly, it’s ad hominem. But secondly, despite how many times you may hear that ‘the science’ says X, the reality is this is a complex issue – particularly with regards to policy responses – with no scientific consensus.
This astroturfed ‘consensus’ narrative has been amplified and enforced via censorship in the media and online. It distorts the true picture of esteemed experts on both sides of this debate. Unfortunately, ‘the science’ is a phrase that has been abused by policy makers to the point where it has lost almost all meaning.
{kind=link}
I would encourage anyone who’s read this far to engage with primary sources (I have tried to link as many as I can in this article) and draw their own conclusions. As so many of my posts on this site emphasise in one way or another: It doesn’t matter who said something – or their credentials, or how many people agree with them – all that matters is the underlying reasons.

“As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.
Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.”
I agree with your article overall. Feel much the same myself, and have been recording relevant ONS stats over the last few months. Psychological Murder (PM) is what we suffering from at the moment.
Brilliant.
I’ve barely seen such a bad research propaganda BS article. It’s full of a lack of evidence, ignore of scientific facts and wrong claims. You should really read a scientific book and educate yourself on evidence based science, pandemy and statistical research.
I’ve really liked to read you articles about coins but you should stop writing medical articles since you have a complete lack of knowledge on medical science and no clue about it in total. It’s like a script kiddie shitcoin which is total crap (Justin Sun) but claims to have solved scalability problems.
I’m sad to say, bro, your article is nightmare uneducated propaganda BS, unfortunately.
2 years on I think my post has aged really well but your comment has not.